


The Game of Trials
Clinical trials are a high stakes game of misaligned incentives. A game theory lens helps us understand why.

** Recently, I had the absolute privilege of moderating a panel with three former FDA Commissioners where the topic was AI and the FDA. We recognized that the conversation made sense only in the grander setting of clinical trial challenges today. That conversation was instrumental in fine tuning my thoughts (and the ultimate thought experiment) below. **
1. Introduction
In the game of R&D, the clinical trial is the final boss. When a trial succeeds, it’s a moment years in the making, and well-worth celebrating. Just look at the trials for the injectable GLP-1 Receptor Agonists, which currently have four branded drugs in market across diabetes, obesity and cardiovascular disease, shared by two pharmaceutical companies (Novo Nordisk and Eli Lilly). Based on those trials and the real-world uptake, Novo and Lilly catapulted themselves into stratospheric market capitalizations. You’d argue these companies played the game well.
But did they really? GLP-1 was discovered in 1986, and the first GLP-1 agonist class drug got approved only in 2005. For the injectable versions which took the market by storm (semaglutide and tirzepatide) more than 35,000 patients were enrolled1, across duplicative studies looking at the same endpoints, with similar inclusion and exclusion criteria. Feels like wasted time and money.
In aggregate, most clinical trials don’t actually have Ozempic-level success. About 90% of all trials fail. Worse, flawed ones sometimes succeed, pushing ineffective or even harmful treatments to market. Also, trials are slow and expensive: In the US, a recent estimate pegged the cost at $117.4 million per approved drug2 - nearly 70% of total R&D spending. The process can take 5-10 years and trust among stakeholders is often in short supply. These costs add up: for sponsors, for the system, and most of all, for patients still waiting for better options.
Expensive, siloed, failure-prone. If someone handed me this “trials” video game on a cartridge in the ‘90s, I’d have just chucked it and walked away from my Nintendo console.
How did we get here? Clinical trials are not purely scientific endeavors; they are also shaped by competitive behaviors among pharmaceutical companies, regulators, research institutions, and patients. Each player has different goals, and their decisions influence one another. Game theory, a mathematical framework developed by von Neumann and Morgenstern (1944), helps explain why the system tends to settle into inefficient outcomes.
A key concept in game theory, the Nash equilibrium - yes, from the “Beautiful Mind” guy - describes a state where no player can improve their position by changing strategy alone (Nash, 1950). Unfortunately, in clinical trials, this equilibrium is often not the best possible outcome for all involved. The system resembles the classic Prisoner’s Dilemma (Axelrod and Hamilton, 1981), where rational actors following their self-interest create inefficiencies that hurt everyone in the long run.
In clinical trials, competitive behaviors like information hoarding, duplicate studies, and strategic participant recruitment may be individually rational, but collectively wasteful3.

What if we could change the rules? What if clinical trials could be structured to encourage collaboration rather than competition? The rest of this article explores how game theory explains current inefficiencies and how a new approach could lead to better outcomes for all stakeholders.
In the deep dive below, we will:
Set the stage with a crash course on game theory concepts and on clinical trial stakeholders
Explore the game dynamics in clinical trials
Argue that Collaboration >> Competition (even if today there are barriers to optimal collaboration)
Set up a thought experiment to remove those barriers and incentivize collaboration (The “Game of Trials”!)
Conclude with some thoughts from an AI in Healthcare FDA Commissioner Panel I recently moderated
This is going to be a long post, but hopefully well-worth it if you’re curious about clinical trials (or just want a little math refresher). As you read it, put yourself in the shoes of a pharma CEO: Would YOU play a fully collaborative game of clinical trials?
2. Game Theory Crash Course
Let’s cover some basics. If you’ve ever played a board game4 or two, some of these concepts will feel intuitive already.
What is game theory?
Game theory is the study of strategic decision-making. It provides us with a framework for understanding how people (or organizations) make decisions when their outcomes depend not just on what they do, but also on what others do (von Neumann and Morgenstern, 1944; Nash, 1950). It’s like chess or poker, but applied to real-world situations like business competition, international relations, and, yes, even clinical trials.
Here’s some fundamental concepts, with clinical trial applications:
Players: These are the decision-makers in a game: individuals or organizations capable of making strategic choices. In clinical trials, players include pharmaceutical companies, regulators, research institutions, and trial participants. Two types of players we’ll often encounter are Principal (who delegates tasks) and Agent (who executes on those tasks).
Strategies: A strategy is a complete plan of action available to a player. It specifies what action the player will take at each decision point. Strategies might include decisions about what data to share, how to design protocols, or whether to publish negative results.
Payoffs: Payoffs represent the value or utility that players receive as a result of the combination of strategies chosen by all players. In clinical trials, payoffs might include regulatory approval, scientific recognition, financial returns, or improved patient outcomes.
Information: Games vary in how much information players have about others' strategies and payoffs. Clinical trials often involve asymmetric information, where some stakeholders know more than others about certain aspects of the process.
Game theory concepts that apply to clinical trials
Nash Equilibrium: A situation where no player benefits by changing their strategy unilaterally (Nash, 1951). This often results in stable, but suboptimal outcomes, such as companies running redundant studies rather than collaborating.
Pareto Optimality: An outcome is Pareto optimal if there’s no way to make someone better off without making someone else worse off (Pareto, 19065). It represents maximum efficiency: the “frontier” of possible outcomes. In trials, the system often settles into a Nash equilibrium that isn’t Pareto optimal. In plain English? We’re stuck in a situation where no single player can improve their position by changing strategy alone, but everyone could be better off if they coordinated their actions. This resembles…
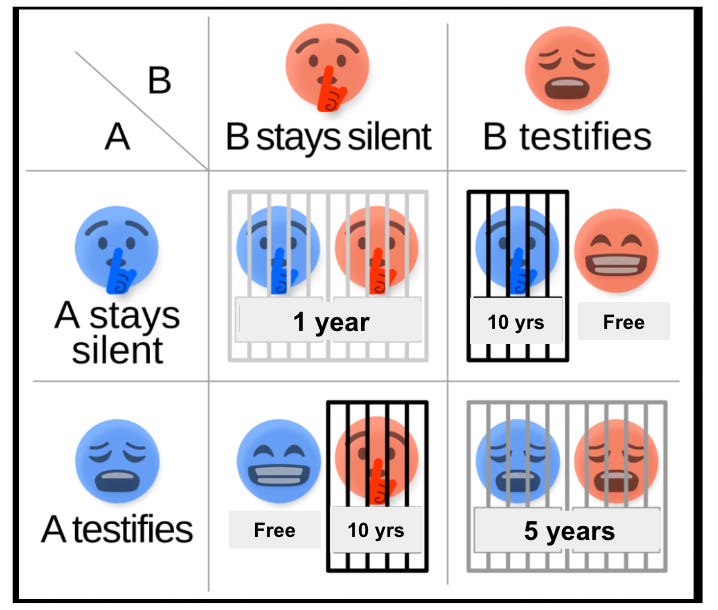
…The Prisoner’s Dilemma: The classic game theory scenario where two suspects are interrogated separately (Tucker, 1950). Each has two options: remain silent (cooperate with their accomplice) or testify (defect). The payoffs create a situation where: If both cooperate, they each get a moderate sentence (1 year). If one defects while the other cooperates, the defector goes free while the cooperator gets a severe sentence (10 years). If both defect, they both get substantial sentences (5 years).
The dilemma? Rational self-interest leads both to defect, resulting in a worse outcome than if they had both cooperated. This illustrates how individual rationality can lead to collective irrationality.
In clinical trials, companies may hoard data and avoid collaboration, even though many would benefit from information sharing.
Beyond the One-Shot Game
This is very important and critical to our thought experiment at the end of this article. The classic Prisoner’s Dilemma assumes a one-time interaction. But in real life, including clinical trials, players interact repeatedly over time. (Axelrod, 1984)
This changes things:
Players can build reputations
Trust becomes valuable
Cooperation can emerge as a stable strategy
“Tit-for-tat” (cooperate first, then mirror the other player’s previous move) can be effective
3. Players in the Clinical Trial Game
Below, I summarize the major players in clinical trials and how their strategic interests influence the system. This is not meant to be a full summary of how a clinical trial runs. If you want a hilarious primer on the topic of trials, please check out Nikhil Krishnan’s children’s book for adults: If you give a mouse metformin. Other writeups that merit further reading: DiMasi and colleagues’ overview of the industry in the Journal of Health Economics (2016), Dan Sfera’s LinkedIn post analysis of the Prisoner’s Dilemma for CROs (2025).

Other players include Institutional Review Boards (IRBs) for ethical oversight, Payers and Health Technology Assessment groups who may influence trial design through coverage decisions, and Patient Advocacy Groups, to represent patient interests and often assist with recruitment. For simplicity, I’m not extensively including them in the game.
Also for the sake of simplicity, I’m not distinguishing here between intervention modality (e.g., small molecule, larger biologic, cell & gene, device, etc.), therapeutic area, or time to market (e.g., first in class, fast follower). That said, these are critical components of strategic decision making, and may merit their own game theory analysis6.
Each of these stakeholders makes strategic decisions based on their own incentives, creating a complex web of interactions that shape how clinical trials unfold.
4. Game Dynamics in Clinical Trials
Now let’s examine how these players interact through various game theory models:
4.1 The Sponsor-CRO Relationship: The Principal-Agent Problem
Sponsors delegate trial execution to CROs, creating a classic principal-agent problem (Eisenhardt, 1989). CROs manage day-to-day operations and may prioritize cost and speed over trial quality. Without aligned incentives, sponsors must invest in monitoring to ensure data integrity, adding inefficiencies to the system. This drives up overall trial costs.
4.2 Sponsor-Sponsor Relationships: Strategic Competition
Sponsors working on similar drugs often avoid collaboration, leading to redundant trials. For example, Novo Nordisk and Eli Lilly conducted parallel GLP-1 studies without shared control arms, prioritizing competitive advantage over efficiency. This mirrors the Prisoner’s Dilemma: acting independently wastes resources that could be saved through coordinated trials.
4.3 Sponsor-Site Relationship: The Recruitment Problem
Many trial sites are paid per patient enrolled, encouraging speed over careful screening. This increases dropout rates and leads to inconsistent data, requiring sponsors to implement costly verification procedures (Halpern et al., 2024). Inclusion drift or patient drift (where clinical trial sites either actively or inadvertently stretch inclusion/exclusion criteria to meet recruitment targets) could be a byproduct of these incentives, and lead to data noise that affect trial integrity7.
4.4. Participant Engagement: The Incentive Mismatch
Trial participants (patients) are essential to trials, but often face high burdens with limited direct benefit that doesn’t offset participation burdens8. In some oncology trials, a study may offer only a marginal improvement, like extending life by a few months. From a sponsor’s view, that might be enough for regulatory approval. But why would a participant join? When patients are treated as active collaborators. with transparency, return of results, and meaningful engagement, their participation becomes more likely, and data quality improves. On the flip-side, it’s how the industry ends up with high loss-to-follow-up rates.
4.5 Multi-Stakeholder Safety Reporting: A Collective Action Problem
All stakeholders benefit from accurate safety data, but individual incentives discourage full transparency. Sponsors fear trial delays, investigators worry about reputational risks, and regulators struggle to enforce timely reporting (Moore et al., 2016).
4.6 Sponsor-Regulator Interaction: Sequential Game
In this sequential game, sponsors move first by designing trials, and regulators respond with approval decisions. Sponsors often optimize for what they expect regulators will accept, rather than for the most meaningful evidence. This can result in trials with less informative endpoints and missed opportunities for better data.
4.7 The Global Clinical Trial Ecosystem: Multi-Player Prisoner’s Dilemma
Sponsors, regulators, investigators, and other stakeholders benefit from shared data and collaborative research infrastructure. However, competitive pressures often lead to siloed efforts, duplicated trials, and delayed publication of negative results. Without coordination mechanisms, each player acts in their own interest, resulting in wasted resources and suboptimal outcomes for patients.
Before we explore how to fix these dynamics, it’s worth asking: what would it take to design a system where collaboration is the rational strategy?
5. Collaboration vs. Competition: Achieving the Global Maximum
Game theory highlights a key tension: stakeholders often pursue competitive strategies, but the greatest collective benefit, if defined as lower costs, more safe and effective drugs to market, and better patient outcomes, comes from collaboration.
Why Collaboration Works
Resource Efficiency: Shared control arms, recruitment, and infrastructure reduce redundancy and improve ROI (Woodcock & Woosley, 2008).
Knowledge Optimization: Open data sharing enables learning from failures, cross-disciplinary insights, and faster methodological innovation (Mello et al., 2013).
Risk Distribution: Collaboration spreads financial and scientific risk, improves design, and enhances safety and regulatory engagement.
Real World Proof
COVID-19 Vaccines: Global coordination led to multiple safe, effective vaccines in under a year, enabled by shared data, public-private funding, and early manufacturing (Lurie et al., 2020).
Rare Disease Models: Groups like the Cystic Fibrosis Foundation and Structural Genomics Consortium show how shared data and patient networks accelerate neglected research (Griggs et al., 2009).
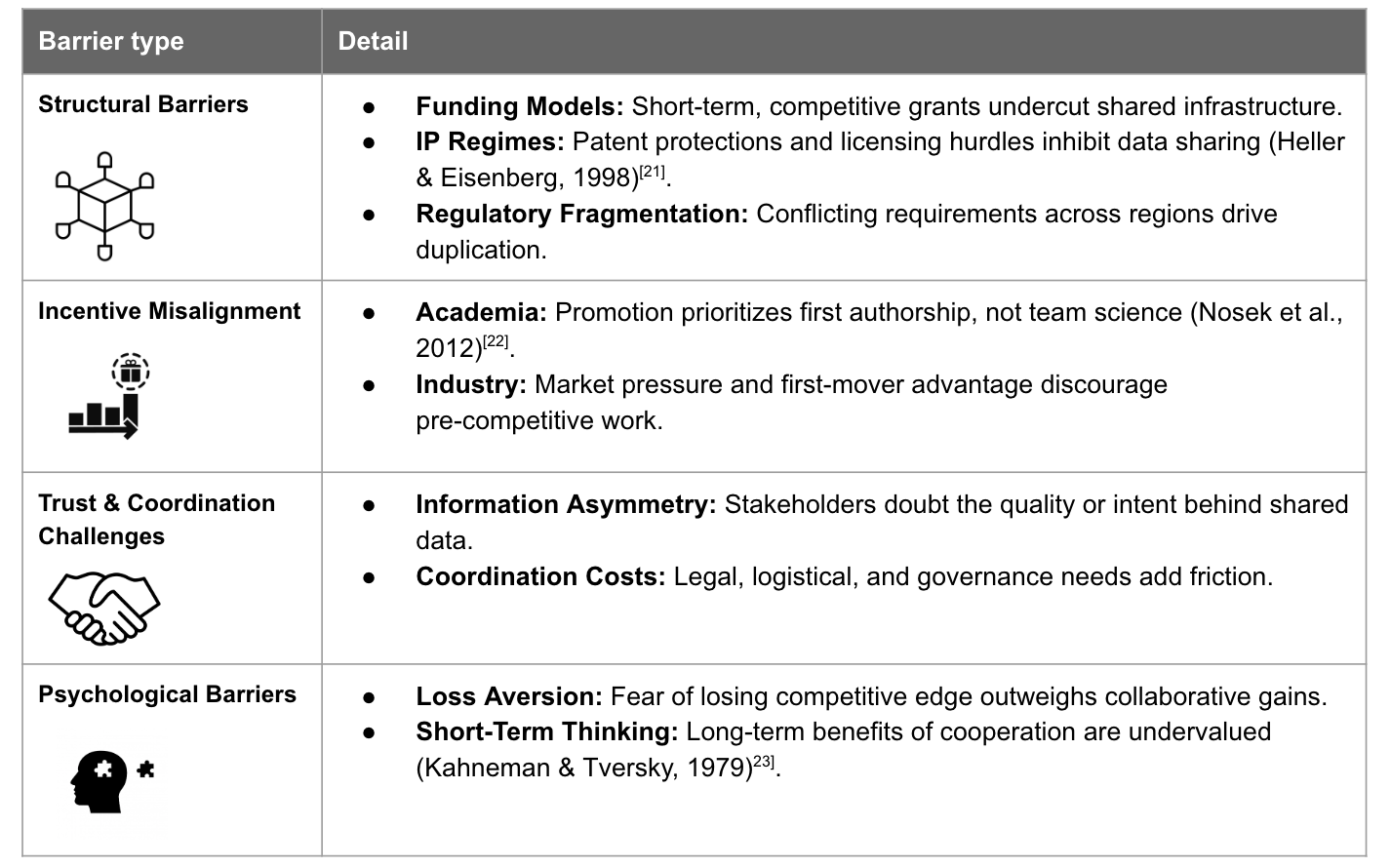
Barriers to Optimal Collaboration
Despite the benefits, real collaboration faces obstacles across systems, incentives, and psychology.
6. Thought Experiment: The Game of Trials
We finally made it to the thought experiment! I’m naming it “Game of Trials9” (GoT, but not the scary one), imagines a future where data, reputation, and scientific rigor are exchanged across an ecosystem of aligned incentives. Rather than relying on altruism or regulation alone, GoT builds a new game where the rational strategy for every stakeholder is to collaborate.
How this could work:
An AI-Powered Trial Engine (with Data Trust Access): The FDA offers an AI search engine trained on all historical regulatory trial data. It helps sponsors design smarter studies and uncover new hypotheses. But access is conditional: sponsors must contribute to a shared Data Trust and agree to participate in joint master protocols for "me too" drugs (Ostrom, 1990). Technologists would need to step up here as well, to provide peace of mind around query exploitation attacks, or other ways in which a bad actor can take advantage of this system.
A Prediction Market for Clinical Trials: A real-time, auditable prediction market lets sponsors, researchers, and patient advocates “bet” or “vote” on trial outcomes and designs. Stakeholders can signal confidence in an intervention or, alternatively, “short” weak science. Failed trials still create value through early insights sold to competitors. The market gives early feedback, distributes risk, and incentivizes transparency (Nowak & Sigmund, 2005).
Reputation & Participation Incentives: Sponsors, CROs, sites, and investigators earn reputation scores based on data quality, transparency, and adherence to collaborative practices. These scores influence future market participation and access to shared infrastructure. Over time, the reputational currency becomes as valuable as traditional IP (Camerer, 2003). Regulators can incorporate additional incentives like “pre-certifications” of certain approaches or protocols, and increased IP protection (say, 15+ years) for innovative trials where all stakeholders collaborate.
Why this could work:
Unlike a one-shot Prisoner’s Dilemma, clinical trials play out as repeated games. The same sponsors, CROs, regulators, and sites interact with each other over and over again. In repeated games, reputation is the name of the game. Cooperation becomes a rational strategy because the long-term benefits of trust and reciprocity outweigh the short-term incentives to defect.
GoT is built around this dynamic. Its mechanisms of AI tools, prediction markets, and reputation incentives should reward consistent, high-quality behavior over time. The more a player collaborates, the more they gain in terms of payoff: access to smarter design tools, early signals from the market, and elevated standing in the research ecosystem.
By structuring collaboration based on transparent information as a winning long-term strategy, the Game of Trials turns cooperation from a gamble into a logical move.

7. Some thoughts from the FDA Commissioner Panel
Back to the Commissioner Panel at the Shaper Capital AI in Healthcare conference that I mentioned in the beginning. While the topic of the conversation was AI and not game theory, the insights shared really helped me refine my thoughts. So, I wanted to highlight a few. They partially support my case, yet show me that a collaborative universe would still be quite a ways away.
The data is out there: FDA, in collaboration with sponsors, trial participants, and the broader trial ecosystem, has access to a treasure trove of data. In an ideal universe, the “AI-Powered Trial Engine” could be feasible. But who gets to make that decision? Who does the data belong to? Is it the FDA, the sponsors, the trial sites, the CROs? Or is it, ultimately, the patients?
Example: even launching clinicaltrials.gov back in the day was difficult, as the information that was required to be shared was considered proprietary information
Broader access to data would also allow us to learn from negative results faster. Remember, 90% of all clinical trials fail. Simplifying a bit, this means we’re not getting access to ~90% of the insight.
Incentives work: While they directionally agreed on aligning towards incentives, the Commissioners diverged on what they would prioritize. I say we do them all: knowledge sharing in exchange for more data access, longer IP protection for the collaborator profile, agile updates in frameworks and guidances. Just as importantly: have incentives that go beyond profit maximization. After all, we’re in this game for improved patient outcomes. There are many other businesses and industries where one can generate outsize returns. There’s something of higher value that gets smart and hardworking people attracted to clinical research and public health.
The chicken and the egg: would a CEO be able to make the case to his or her board to do a collaborative trial on a major asset? Even if “the math” proves this to be true, there are still many barriers to putting this into practice. It is difficult to be the first one to agree to this.

8. Conclusion
Clinical trials currently function as a suboptimal game, where rational self-interest leads to inefficiencies that slow progress and increase costs. By restructuring incentives, we can shift from a Prisoner’s Dilemma to a Coordination Game, where cooperation benefits all players.
The COVID-19 vaccine race demonstrated that collaboration accelerates breakthroughs (Lurie et al., 2020). A permanent shift toward structured cooperation could deliver faster, safer, and more cost-effective clinical trials. The key takeaway? Aligning incentives correctly can lead to a better system, not through altruism, but by making collaboration the most rational choice.
Would you play the game?
Would I? If I were a pharma or biotech CEO (and I hope to someday be!) I would have a hard time convincing my board to go for a collaborative trial, unless the incentives were truly incredible, e.g., if my company and my competitors were racing to something completely game-changing, AND the FDA and other regulators gave us, say, 2x the patent protection time as a reward for collaboration, AND worked with us hand-in-hand in data sharing and clearly spelling out all the trial expectations. Once such a collaborative consortium succeeds, many others would follow. In my experience with pharma and biotech, no one wants to be first, but no one wants to be third.
That’s all for now! 💭
Acknowledgements: Special thanks to Dr. Robert Califf, Dr. Steve Hahn and Dr. Andrew von Eschenbach for the on-stage discussion which helped me refine this article. Thank you to Karin E, Max W, Mike B, and Nate B for feedback on this article. This writeup got some major assists from non-humans, too: tthanks to Manus AI (for the nerdy academic parts, and for wrangling and formatting the right citations) and ChatGPT (for back-and-forth ideation on the thought experiment and for copy-editing). Most of the ideation with AI deep research did not make it into this writeup. Turns out AI models are even more verbose than I am! But it made for some interesting learnings for me.
9. References
von Neumann, J., & Morgenstern, O. (1944). Theory of games and economic behavior. Princeton University Press.
Nash, J. (1950). Equilibrium points in n-person games. Proceedings of the National Academy of Sciences, 36(1), 48-49.
Axelrod, R., & Hamilton, W. D. (1981). The evolution of cooperation. Science, 211(4489), 1390-1396.
Nash, J. (1951). Non-cooperative games. Annals of Mathematics, 54(2), 286-295.
Pareto, V. (1906). Manuale di economia politica. Societa Editrice.
Tucker, A. W. (1950). A two-person dilemma. Unpublished notes, Stanford University.
Axelrod, R. (1984). The evolution of cooperation. Basic Books.
DiMasi, J. A., Grabowski, H. G., & Hansen, R. W. (2016). Innovation in the pharmaceutical industry: New estimates of R&D costs. Journal of Health Economics, 47, 20-33.
Sfera, D. (2025). The Prisoner’s Dilemma amongst contract research organizations (CROs). LinkedIn Pulse.
Lidz, C. W., Appelbaum, P. S., Grisso, T., & Renaud, M. (2012). Therapeutic misconception and the appreciation of risks in clinical trials. Social Science & Medicine, 58(9), 1689-1697.
FDA. (2018). Clinical trial conduct: GCP questions and answers. Food and Drug Administration.
Eisenhardt, K. M. (1989). Agency theory: An assessment and review. Academy of Management Review, 14(1), 57-74.
Halpern, S. D., Karlawish, J. H., & Berlin, J. A. (2024). Optimizing patient recruitment for clinical trials: A hybrid classification model and game-theoretic approach for strategic interaction. IEEE Access.
Moore, T. J., Furberg, C. D., Glenmullen, J., Maltsberger, J. T., & Singh, S. (2016). Suicidal behavior and depression in smoking cessation treatments. PLoS ONE, 6(11), e27016.
Longo, D. L., & Drazen, J. M. (2016). Data sharing. New England Journal of Medicine, 374(3), 276-277.
Woodcock, J., & Woosley, R. (2008). The FDA critical path initiative and its influence on new drug development. Annual Review of Medicine, 59, 1-12.
Mello, M. M., Francer, J. K., Wilenzick, M., Teden, P., Bierer, B. E., & Barnes, M. (2013). Preparing for responsible sharing of clinical trial data. New England Journal of Medicine, 369(17), 1651-1658.
Lurie, N., Saville, M., Hatchett, R., & Halton, J. (2020). Developing Covid-19 vaccines at pandemic speed. New England Journal of Medicine, 382(21), 1969-1973.
Griggs, R. C., Batshaw, M., Dunkle, M., Gopal-Srivastava, R., Kaye, E., Krischer, J., Nguyen, T., Paulus, K., & Merkel, P. A. (2009). Clinical research for rare disease: Opportunities, challenges, and solutions. Molecular Genetics and Metabolism, 96(1), 20-26.
Heller, M. A., & Eisenberg, R. S. (1998). Can patents deter innovation? The anticommons in biomedical research. Science, 280(5364), 698-701.
Nosek, B. A., Spies, J. R., & Motyl, M. (2012). Scientific utopia: II. Restructuring incentives and practices to promote truth over publishability. Perspectives on Psychological Science, 7(6), 615-631.
Kahneman, D., & Tversky, A. (1979). Prospect theory: An analysis of decision under risk. Econometrica, 47(2), 263-291.
Ostrom, E. (1990). Governing the commons: The evolution of institutions for collective action. Cambridge University Press.
Nowak, M. A., & Sigmund, K. (2005). Evolution of indirect reciprocity. Nature, 437(7063), 1291-1298.
Camerer, C. F. (2003). Behavioral game theory: Experiments in strategic interaction. Princeton University Press.
Author analysis based on numbers shared for Novo Nordisk’s published data on SUSTAIN, PIONEER, and STEP trials, and Eli Lilly’s SURPASS and SURMOUNT trials.
Accounting for failures along the way, and for cost of capital.
So many people in the clinical trial industry make their careers and a living around implementing these “individually rational, collectively wasteful” decisions. Fixing the trial issues might leave them out of a job, the implications of which are a discussion well worth having.
Anyone want to build a Clinical Trials board game?! Dead serious about this, call me.
This is a whole 600 page book, and it’s in dense Italian, so I don’t recommend you actually read it. But wouldn’t it be fun if you were able to (without AI translation help)? Teasing here that I’ll have a fun blog post on language learning coming up soon.
Market share dynamics in crowded drug classes (e.g., GLP-1s, immunotherapies) involve some serious “say it with charts” efforts. Like charts? Let me know if you’d like to collaborate on that follow-up post!
There are multiple root causes for this kind of inadvertent enrollment inflation. Pressure to meet enrollment targets could be a big one, but I also see lack of clarity in inclusion / exclusion criteria and the general belief that the patient might still benefit or qualify if the criteria were interpreted more liberally as impacting this one. Overall, I don’t think inclusion drift comes from malicious intentions.
On average, a clinical trial site is 60 miles away from the participant. That was exactly the distance I had to commute (via some very expensive Uber rides!) for the first clinical trial I participated in.
Call me “mother of trials” but give me a better ending.
Really interesting analysis of the incentives of clinical trials! Having that many stakeholders definitely makes solving for optimality very complex, but lots of room for improvement from how things are done now. I don't know a lot about how clinical trials are run but while researching gene and cell therapies for an essay I learned about the RMAT designation and accelerated approval pathway, which has a mechanism for pooling data (for similar manufacturing protocols), which allows small sponsors to basically run trials together. I wonder if similar structural mechanisms can be extended to trials outside gene and cell therapies?
Also, the mention of game theory and repeated games reminded me of this incredible "game" (explorable explanation) by Nicky Case. Very useful for understanding the complex mechanisms behind the theory: https://ncase.me/trust/
Fascinating article. Given the recent rise of China as a source of innovation (documented on Biotech hangout for example), I wonder if this collaborative approach may gain traction (necessity being the mother of invention). One of China’s advantages is the ability to significantly accelerate both pre-clinical and early clinical trials vs US. Now the downside of such an approach which prioritises speed above all else, may be trial quality.